A lower limb prosthetic device (prosthesis) has the main purpose of replacing the rest of the limb, joints and foot following limb loss, or filling the space between the end of a congenital limb difference and the ground. The ideal outcome is a well-fitting prosthetic leg, that distributes pressures evenly, with the forces going through the limb and components optimally to enable improved mobility.

Mobility is different for everyone – transfers, walking around the shops, hanging out the washing, running 5km, office jobs or farming, everyone has different interests, goals and daily activities. No matter your lifestyle or goals, the ForMotion team will help you on the way to meeting and hopefully exceeding your potential.
There are two main categories of function of prosthetic legs
Mechanical – Using the built in properties of the device and components along with your body movements to get the function out of the prosthesis.
Microprocessor – Computer controlled movement.
In recent years there has been development in Powered lower limb prosthetic componentry. Take a look at our resources to learn some advancements in prosthetic technology.
See below to learn a little bit about different levels of amputation/limb difference and some examples of what a prosthetic leg design could look like. Talk to your prosthetist if you have specific activities or movements that you can’t do with your prosthesis, as you may need a specialty prosthesis.



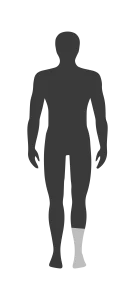 Trans-tibial means cut through the tibia (shin bones). This is how your doctors, physiotherapists and prosthetist will often refer to a below knee amputation or below knee prosthesis.
Trans-tibial means cut through the tibia (shin bones). This is how your doctors, physiotherapists and prosthetist will often refer to a below knee amputation or below knee prosthesis.
Retaining the anatomical knee joint means that a lot less effort is required to walk with this style of amputation compared to higher levels of amputation. As there is no weight bearing bone remaining, the soft tissue is loaded to take the weight when standing/walking

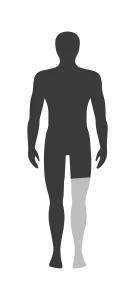 Trans-femoral means cut through the femur (thigh bone). This is how health professionals refer to an above knee amputation or above knee prosthesis.
Trans-femoral means cut through the femur (thigh bone). This is how health professionals refer to an above knee amputation or above knee prosthesis.
Above knee prosthetic legs require the user to use their muscles to control the prosthetic knee (even with an MPK or powered knee). See our resource on the difference between prosthetics and bionics to learn more. The socket is designed to provide stability at the hip and help the wearer stay vertical. There are many socket designs, speak to your prosthetist if something is not right, you may need to try something new!

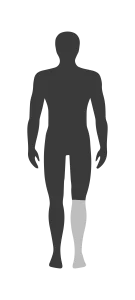 Knee disarticulation amputation means through the knee joint, no bones are cut in this style of amputation. Though sometimes the condyles are shaved.
Knee disarticulation amputation means through the knee joint, no bones are cut in this style of amputation. Though sometimes the condyles are shaved.
Through knee amputees retain a weight bearing surface, and a long lever arm makes walking easier for many compared to above knee amputees. However, the knee centre is no longer in line with the sound side which can lead to asymmetrical gait and a longer limb when sitting. Due to the stump being bigger at the bottom, your socket design will either need to involve build ups or adjustable panels to allow you to get into the prosthetic leg. If your condyles have been shaved, then this is not always necessary.

 We use partial foot to generalise the many kinds of amputation and limb difference that can occur at the level of the toes/feet. You could be missing the entire first ray, be complete trans-metatarsal or have a chopart amputation – retaining only the heel. Sometimes we may group toe amputations into this category, though they are technically their own level of amputation.
We use partial foot to generalise the many kinds of amputation and limb difference that can occur at the level of the toes/feet. You could be missing the entire first ray, be complete trans-metatarsal or have a chopart amputation – retaining only the heel. Sometimes we may group toe amputations into this category, though they are technically their own level of amputation.
There are many prosthetic options available for partial foot amputees. From silicone cosmetic restoration to devices incorporating carbon AFOs to gain additional stability and spring. Even ‘cosmetic’ prosthetics have a functional benefit to the wearer. A single toe prosthesis can help keep remaining toes and bones in the foot in alignment, prevent excessive pressures on the foot, that can lead to rubs and further amputation.

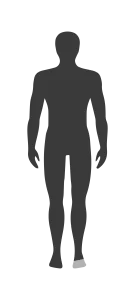
 Symes is more commonly used term to describe an ankle disarticulation amputation. No bones are cut with a symes amputation, with the patient retaining the full tibia and fibula (shin bones).
Symes is more commonly used term to describe an ankle disarticulation amputation. No bones are cut with a symes amputation, with the patient retaining the full tibia and fibula (shin bones).
Many symes prosthetic users are able to retain weight bearing ability through the end of their stump/residual limb. The long lever arm of the remaining limb means you can often have lower trim lines of the socket, freeing up knee range of motion. Due to the stump being bigger at the bottom, your socket design will either need to involve build ups or adjustable panels to allow you to get into the prosthetic leg.

 Hip Disarticulation is an amputation through the hip joint, where the entire lower limb is removed. No bones are cut in this style of amputation. If the surgery included part of the pelvis, this is called a hindquarter amputation or hemipelvectomy.
Hip Disarticulation is an amputation through the hip joint, where the entire lower limb is removed. No bones are cut in this style of amputation. If the surgery included part of the pelvis, this is called a hindquarter amputation or hemipelvectomy.
This level of amputation requires the most amount of energy and concentration to walk as there are 2 joints (the prosthetic hip and prosthetic knee) and the prosthetic foot that need to be controlled. People with this style of prosthetic leg have to have a unique gait technique to get the optimal function out of the prosthesis.

 Congenital limb difference presents in many unique ways, at all levels of the limb. Some differences present at the foot only, could be congenital symes, tibial hemimelia, PFFD and many more. Within each of these diagnoses, no two people are the same. Some congenital patients or those with osteosarcoma go through surgeries to remove the affected area. Rotationplasty has been becoming more common as a solution to both osteosarcoma and various congenital presentations.
Congenital limb difference presents in many unique ways, at all levels of the limb. Some differences present at the foot only, could be congenital symes, tibial hemimelia, PFFD and many more. Within each of these diagnoses, no two people are the same. Some congenital patients or those with osteosarcoma go through surgeries to remove the affected area. Rotationplasty has been becoming more common as a solution to both osteosarcoma and various congenital presentations.
As a parent, or as someone born this way, the ForMotion team is dedicated to finding a solution that is as unique as you are.



